Index
Atrioventricular Communication
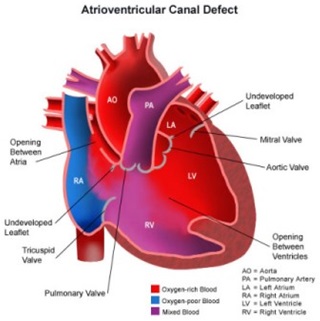
What Is Atrioventricular Communication?
Atrioventricular septal defect (AVSD) or atrioventricular canal defect (AVCD), also known as
"Common Atrioventricular Canal" abbreviated as (CAVC) or "Endocardial Cushion Defect" abbreviated as (ECD),
is characterized by a deficiency of the atrioventricular septum of the heart.
What Causes Atrioventricular Communication?
It is caused by an abnormal or inadequate fusion of the superior and inferior endocardial cushions with
the mid portion of the atrial septum and the muscular portion of the ventricular septum.

What are the Signs & Symptoms of Atrioventricular Communication?
Symptoms include difficulty breathing (dyspnoea) and bluish discoloration on skin and lips (cyanosis).
A newborn baby will show signs of heart failure such as edema, fatigue, wheezing, sweating and irregular heartbeat.
HEART CONDITIONS Diseases and Treated FAQ's
AVSDs can be detected by cardiac auscultation; they cause atypical murmurs and loud heart tones.
Confirmation of findings from cardiac auscultation can be obtained with a cardiac ultrasound (echocardiography - less invasive) and cardiac catheterization (more invasive).
Tentative diagnosis can also be made in utero via fetal echocardiogram.
An AVSD diagnosis made before birth is a marker for Down syndrome, although other signs and further testing are required before any definitive confirmation of either can be made.
Confirmation of findings from cardiac auscultation can be obtained with a cardiac ultrasound (echocardiography - less invasive) and cardiac catheterization (more invasive).
Tentative diagnosis can also be made in utero via fetal echocardiogram.
An AVSD diagnosis made before birth is a marker for Down syndrome, although other signs and further testing are required before any definitive confirmation of either can be made.
Treatment is surgical and involves closure of the atrial and ventricular septal defects and restoration of
a competent left AV valve as far as is possible. Open surgical procedures require a heart-lung machine and are done with
a median sternotomy.
Surgical mortality for uncomplicated ostium primum defects in experienced centers is 2%; for uncomplicated cases of complete atrioventricular canal defect, 4% or less. Certain complications such as tetralogy of Fallot or highly unbalanced flow across the common AV valve can increase risk significantly.
Infants born with AVSD are generally in sufficient health to not require immediate corrective surgery.
If surgery is not required immediately after birth, the newborn will be closely monitored for the next several months, and the operation held-off until the first signs of lung distress or heart failure. This gives the infant time to grow, increasing the size of, and thereby the ease of operation on, the heart, as well as the ease of recovery. Infants will generally require surgery within three to six months, however, they may be able to go up to two years before the operation becomes necessary, depending on the severity of the defect.
Surgical mortality for uncomplicated ostium primum defects in experienced centers is 2%; for uncomplicated cases of complete atrioventricular canal defect, 4% or less. Certain complications such as tetralogy of Fallot or highly unbalanced flow across the common AV valve can increase risk significantly.
Infants born with AVSD are generally in sufficient health to not require immediate corrective surgery.
If surgery is not required immediately after birth, the newborn will be closely monitored for the next several months, and the operation held-off until the first signs of lung distress or heart failure. This gives the infant time to grow, increasing the size of, and thereby the ease of operation on, the heart, as well as the ease of recovery. Infants will generally require surgery within three to six months, however, they may be able to go up to two years before the operation becomes necessary, depending on the severity of the defect.
Down syndrome is often associated with AVCD.
Other risk factors include: having a parent with a congenital heart defect, alcohol use while pregnant, uncontrolled diabetes
treatment during pregnancy and some medications during pregnancy.
This type of congenital heart defect is associated with patients with Down syndrome (trisomy 21) or heterotaxy syndromes.
45% of children with Down syndrome have congenital heart disease. Of these, 35–40% have AV septal defects. Similarly, one-third of all children born with AVSDs also have Down syndrome.
A study also showed that there is also an increased risk of atrioventricular canal in patients who suffer from Noonan syndrome.
The pattern seen in those patients with Noonan syndrome differ from those patients who have Down syndrome in that "partial" AVCD is more prevalent in those who suffer from NS, where as those who suffer from down syndrome show a prevalence of the "complete" form of AVCD.
This type of congenital heart defect is associated with patients with Down syndrome (trisomy 21) or heterotaxy syndromes.
45% of children with Down syndrome have congenital heart disease. Of these, 35–40% have AV septal defects. Similarly, one-third of all children born with AVSDs also have Down syndrome.
A study also showed that there is also an increased risk of atrioventricular canal in patients who suffer from Noonan syndrome.
The pattern seen in those patients with Noonan syndrome differ from those patients who have Down syndrome in that "partial" AVCD is more prevalent in those who suffer from NS, where as those who suffer from down syndrome show a prevalence of the "complete" form of AVCD.