Index
Anomalous Pulmonary Venus
What Is Anomalous Pulmonary Venus?
Anomalous pulmonary venous connection (or anomalous pulmonary venous drainage or anomalous pulmonary venous return) is a congenital defect of the pulmonary veins.
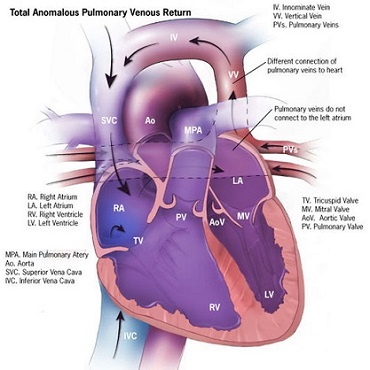
Total Anomalous Pulmonary Venous Connection, also known as total anomalous pulmonary venous return, is a rare cyanotic congenital heart defect in which all four pulmonary
veins are mal positioned and make anomalous connections to the systemic venous circulation.
(Normally, pulmonary veins return oxygenated blood from the lungs to the left atrium where it can then be pumped to the rest of the body).
A patent foramen ovale, patent ductus arteriosus or an atrial septal defect must be present, or else the condition is fatal due to a lack of systemic blood flow. In some cases, it can be detected prenatally.
There are four variants
- Supra-cardiac (50%) : Blood drains to one of the innominate veins (brachiocephalic veins) or the superior vena cava.
- Cardiac (20%): Where blood drains into coronary sinus or directly into right atrium.
- Infra-diaphragmatic (20%): Where blood drains into portal or hepatic veins; and a mixed (10%) variant.
- TAPVC can occur with obstruction, which occurs when the anomalous vein enters a vessel at an acute angle and can cause pulmonary venous hypertension and cyanosis because blood cannot enter the new vein as easily.
(Normally, pulmonary veins return oxygenated blood from the lungs to the left atrium where it can then be pumped to the rest of the body).
A patent foramen ovale, patent ductus arteriosus or an atrial septal defect must be present, or else the condition is fatal due to a lack of systemic blood flow. In some cases, it can be detected prenatally.
There are four variants
- Supra-cardiac (50%) : Blood drains to one of the innominate veins (brachiocephalic veins) or the superior vena cava.
- Cardiac (20%): Where blood drains into coronary sinus or directly into right atrium.
- Infra-diaphragmatic (20%): Where blood drains into portal or hepatic veins; and a mixed (10%) variant.
- TAPVC can occur with obstruction, which occurs when the anomalous vein enters a vessel at an acute angle and can cause pulmonary venous hypertension and cyanosis because blood cannot enter the new vein as easily.
What Causes Anomalous Pulmonary Venus?
This is a congenital defect of the pulmonary veins, not causes are known or associate whit this disease.

What are the Signs & Symptoms of Anomalous Pulmonary Venus?
Right Ventricular heave
- Loud S1,
- Fixed split S2,
- S3 gallop,
- Cardiomegaly,
- Snowman on chest radiograph,
- Cyanosis, tachypnea, dyspnea since the overloaded pulmonary circuit can cause pulmonary edema,
- Cottage-loaf sign, that is, chest X-ray appearance similar to a cottage loaf, also known as the ‘snow man’ sign or ‘figure of 8’ sign.
- Systolic ejection murmur at left upper sternal border,
- Right axis deviation on ECG,
- Right ventricular hypertrophy,
- Loud S1,
- Fixed split S2,
- S3 gallop,
- Cardiomegaly,
- Snowman on chest radiograph,
- Cyanosis, tachypnea, dyspnea since the overloaded pulmonary circuit can cause pulmonary edema,
- Cottage-loaf sign, that is, chest X-ray appearance similar to a cottage loaf, also known as the ‘snow man’ sign or ‘figure of 8’ sign.
- Systolic ejection murmur at left upper sternal border,
- Right axis deviation on ECG,
- Right ventricular hypertrophy,
HEART CONDITIONS Diseases and Treated FAQ's
It can be diagnosed with CT scan, Angiography, Transesophageal Echocardiography,
or cardiac MRI. Unfortunately, less invasive and expensive testing, such as Transthoracic Echocardiography
and CT scanning are generally less sensitive.
TOTAL Anomalous Pulmonary Venus Connection
- In T-APVC without obstruction, surgical redirection can be performed within the first month of life.
The operation is performed under general anesthesia. The four pulmonary veins are reconnected to the left atrium, and any associated heart defects such as atrial septal defect, ventricular septal defect, patent foramen ovale, and/or patent ductus arteriosus are surgically closed. With obstruction, surgery should be undertaken emergently.
PGE1 should be given because a patent ductus arteriosus allows oxygenated blood to go from the circulation of the right heart to the systemic circulation.
PARTIAL Anomalous Pulmonary Venus Connection
- In P-APVCIt is sometimes treated with surgery, which involves rerouting blood from the right atrium into the left atrium with a patch or use of the Warden procedure.
However, interest is increasing in catheter-based interventional approaches, as well as medical therapy for less severe cases.
- In T-APVC without obstruction, surgical redirection can be performed within the first month of life.
The operation is performed under general anesthesia. The four pulmonary veins are reconnected to the left atrium, and any associated heart defects such as atrial septal defect, ventricular septal defect, patent foramen ovale, and/or patent ductus arteriosus are surgically closed. With obstruction, surgery should be undertaken emergently.
PGE1 should be given because a patent ductus arteriosus allows oxygenated blood to go from the circulation of the right heart to the systemic circulation.
PARTIAL Anomalous Pulmonary Venus Connection
- In P-APVCIt is sometimes treated with surgery, which involves rerouting blood from the right atrium into the left atrium with a patch or use of the Warden procedure.
However, interest is increasing in catheter-based interventional approaches, as well as medical therapy for less severe cases.